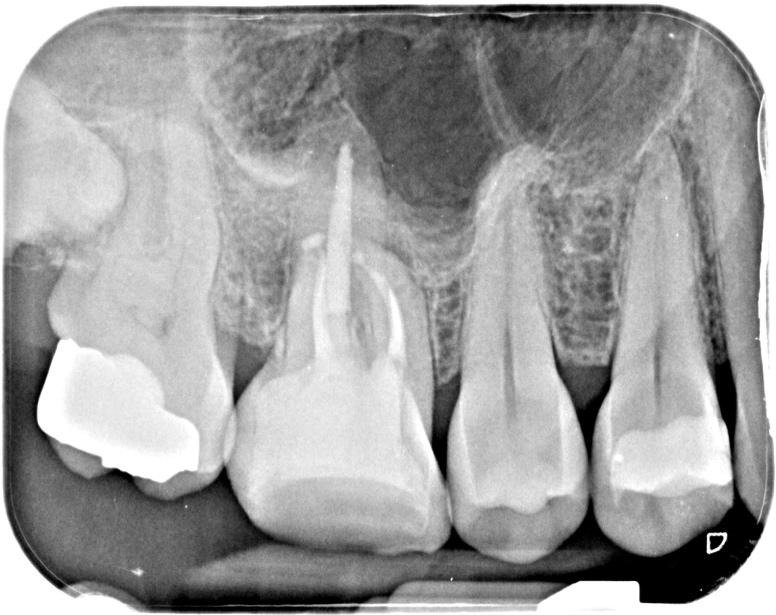
Pre-op IOPA

‘Sometimes it really does pay to keep an open mind.’ This was initially sent to me as a file retrieval case. I think when the referral letter indicates there is a broken file, its easy to become influenced by this and develop ‘tunnel vision’ in the way that you view it. A fresh pair of eyes is often beneficial. I asked Simon Barnwell (Simply endo mentor) for his opinion and he felt this did not look like a broken file in the mesial root. A CBCT scan was taken to help assess the restorability of this tooth and showed the following:
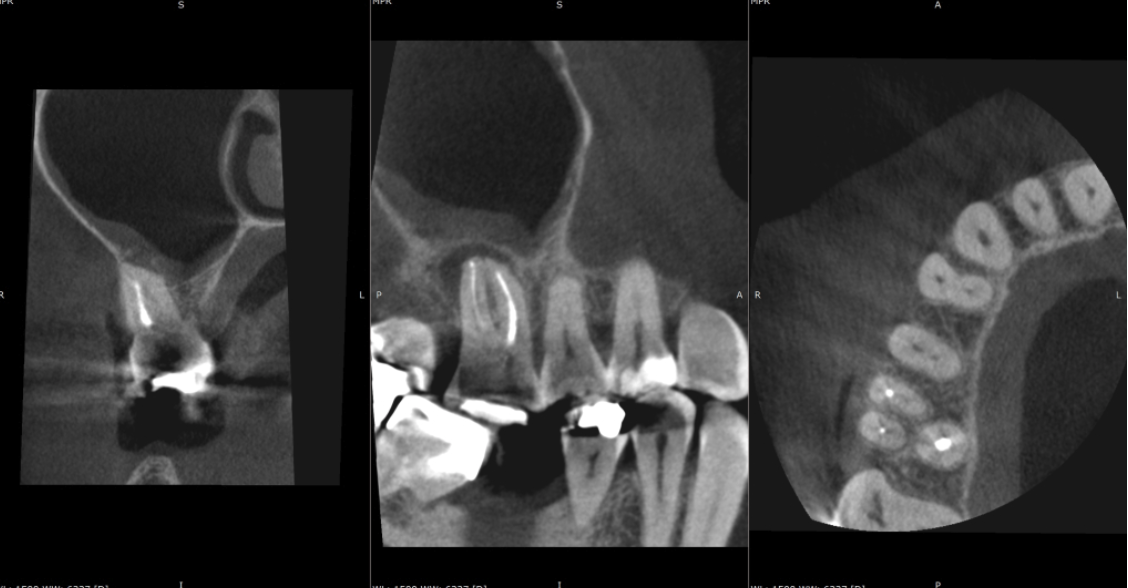
Key findings from CBCT Consultant radiologist’s report by JM Radiology:
- No evidence of a fractured file in the mesial root.
- Vertucci type VI 2-1-2 canal configuration in the mesial root (5-20% of upper first molars are thought to have this canal configuration which is potentially high, so we need to be on the lookout for it!)
- Unfilled mb2 canal
- No signs of PAP on the palatal root (this information became relevant as the treatment progressed)
The information provided by the CBCT made the management of this case far more predictable and allowed me to plan a strategy that would best suit this tooth’s anatomy. This treatment was completed over 2 visits (each visit approximately 90 minutes long). A caries-led access uncovered cracks in the mesial and distal walls that extended into the pulp chamber but stopped before crossing the base of the tooth. Read the latest guidance on the endodontic management of cracked teeth here.
As a result, the cracks were not deemed detrimental to the treatment outcome but were included in the patient’s consent and also highlighted the need for cuspal coverage straight after re-treatment in order to protect the tooth. A pre-endo build-up in 3M’s Filtek Bulk One composite helped seal these cracks beforehand. The re-root treatment was then completed using Reciproc Blue R25, VDW Rotate 2504 for the mb2 and R40 for the wider palatal canal. Following copious irrigation and lots of activation, the canals were obturated using a combination of a squirt fill technique with Totalfill BC sealer Hiflow to try and negotiate the 2-1-2 configuration apically in the mesial root and CWC in the other roots. Patency was not achieved in the palatal root. However, due to the absence of any obvious inflammatory change attached to this root on the pre-op CBCT scan it is less likely to affect the outcome of this case. This patient was then returned to their RD for cuspal coverage without delay!
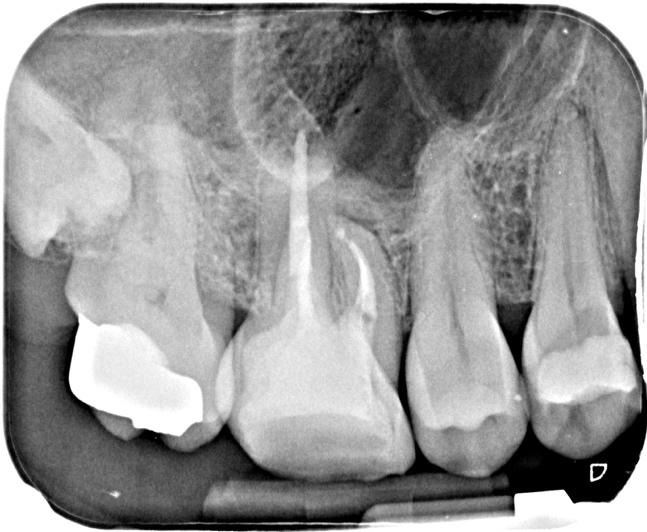
Post-op IOPA’s
I have suggested a follow up CBCT scan in 12 months’ time to assess healing in 3D, especially as this case had been diagnosed and planned in 3D. I’ll add this to the case once I have it.
With the option for self-referrals and referrals by your dentist, Modern Endodontics by Dr Adam Watt makes it easy for root canal patients based in Glasgow and further afield to access advanced endodontic care.
If you're a patient looking to self-refer for an endodontic treatment with Dr Adam Watt, please contact the Treatment Coordinator at Broomhill Dental, Glasgow.